





HEART Pathway
Über HEART Pathway
A validated clinical decision tool for patients presenting to the emergency department with chest pain, created by Wake Forest University School of Medicine physicians. For patients presenting with chest pain, the HEART Pathway algorithm has been shown to reduce patient length of stay by 12 hours, reduce cost by 14 percent per patient, and results in a MACE rate of < 1%.
If interested in licensing the HEART Pathway for use at your institution please contact us via our website.
HEART Pathway randomized controlled trial: http://www.ncbi.nlm.nih.gov/pubmed/25737484
Chest pain is a top cause of US ED visits. Eight to ten million patients with chest pain present to an ED annually in the United States. More than half of Emergency Department patients with chest pain receive lengthy cardiac evaluations in an chest pain unit or inpatient ward, with an annual cost $10-13 billion. Less than ten percent of patients have an acute coronary syndrome (ACS). Two to five percent of patients with myocardial infarctions are inappropriately discharged from the ED every year. Missed ACS is a top cause of malpractice claims.
What is the HEART Pathway?
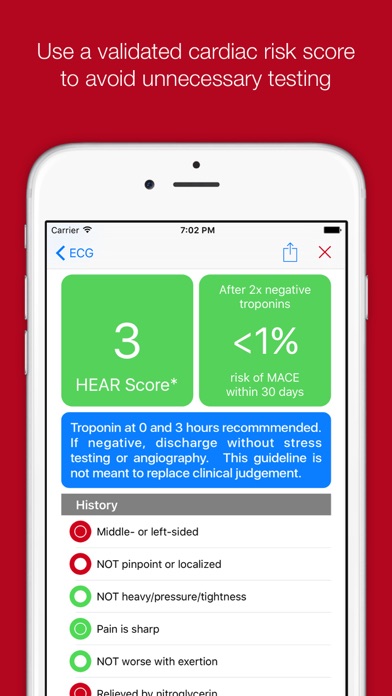
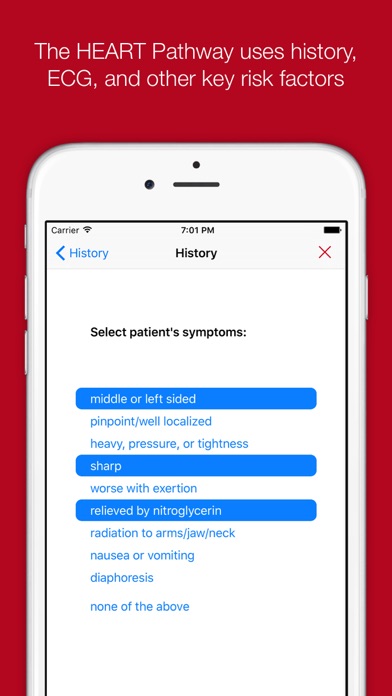
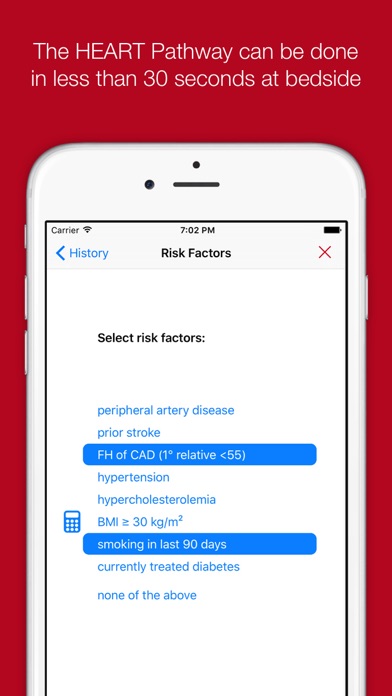
The HEART Pathway is designed for more accurate cardiac risk stratification for patients presenting to the ER with Chest Pain. The HEART Pathway is similar to the HEART Score but has been modified by researchers at Wake Forest University School of Medicine.
The HEART Pathway has been validated by researchers at Wake Forest University School of Medicine and is used on a daily basis at Wake Forest and our affiliate emergency departments.
The HEART Pathway randomized controlled trial (Mahler et al, Circ CVQO J, 2015.) has demonstrated the benefits of the HEART Pathway compared with usual care. When HEART Pathway was applied to chest pain patients researchers found an increase in early discharge rate from 18% to 39% with a cost savings of over $200 per patient.
The HEART Pathway assists providers with answering the following questions:
Should I admit my patient for stress testing or can I discharge my patient from the Emergency Room?
What is the likelihood that my patient’s presenting symptoms represent ACS?
What is the likelihood that my patient will have an ACS event in the near future (within 30 days)?
Bilder

Download




